How one gets liver cancer is a complex multi-step process [1]. It involves damage from inflammation as known as swelling, hepatocyte necrosis and regeneration as well as fibrotic deposition [1]. Inflammation is a response of the body to damage [2]. Inflammation is a protective measure that causes redness, warmth and edema [2]. Necrosis refers to the death of organ tissues. Fibrotic deposition is the formation of scar tissue rather than healthy tissue [2]. This damage to the liver results in cirrhosis which is a large factor in causing carcinoma [1]. All of these alterations in the liver creates an environment where genetic changes may result in liver cancer [1]. However, underlying causes that allows for liver cancer to occur varies depending on the risk factors involved [3].

Shutterstock. (2019). 14 things you need to know about playing beer. Retrieved from https://www.tasteofhome.com/collection/how-to-drink-beer-the-right-way/
|
Alcohol
The liver is responsible for filtering alcohol in the body [2]. The risk of developing liver cancer from alcohol consumption is dependent on the amount of intake in one's lifetime [6]. For the liver to deal with alcohol, it breaks it down into a different form called acetaldehyde [7]. However, this form can actually cause damage to the DNA of the liver cells which increases the risk of cancer [7]. Normally, the liver is able to handle the acetaldehyde and prevent excessive damage [7]. In the case of heavy alcoholics, too much acetaldehyde is formed for the liver to handle in a timely manner which results in cell damage [7]. Additionally, heavy alcohol consumption leads to liver cirrhosis [3]. |
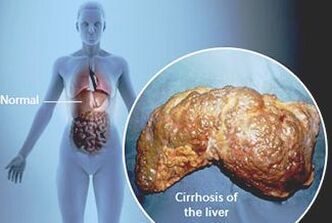
Getty Image (2018) Cirrhosis. Retrieved from https://www.medicinenet.com/cirrhosis/article.htm
|
Cirrhosis
The main characteristics of cirrhosis are decreased hepatocyte replication, which is the main cell of the liver, increased fibrous tissue and destruction of liver cells [3]. Hepatocytes of a liver with cirrhosis have changes in their genes [3]. Their telomeres, the DNA at the ends of chromosomes, are shortened [2,3]. Telomeres are non-functional DNA sequences at the end of cells that are used as a shield against loss of functional DNA [2]. All the effects on the liver from cirrhosis (ie. the inflammation, decreased cell replication, fibrous tissue and the effect of the telomeres) cause an increased chance of tumor and cancer formation [3]. |
1MD. (2019). Non-alcoholic fatty liver disease: Risk, tips, & more. Retrieved from https://1md.org/article/fatty-liver-disease-nafld-risks-tips
|
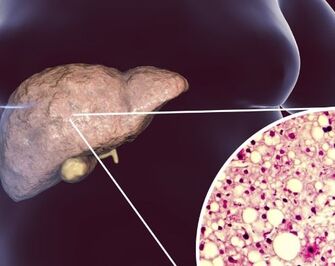
Non-Alcoholic Fatty Liver Disease
This condition refers to the excess buildup of fat in the liver [3]. The main causes of non-alcoholic fatty liver disease (NAFLD) are obesity and diabetes [3]. Obesity and diabetes typically results in insulin resistance [3]. Insulin is a hormone in the body that orders cells to absorb glucose (a sugar) from the blood stream [2]. When the cells are insulin resistant that means they are not absorbing glucose which is needed to function [2]. Fat is then used instead of glucose [2]. The extra fat molecules in the blood are taken up by the liver [3]. The fatty liver causes inflammation and scar tissue formation leading to cirrhosis eventually possibly becoming liver cancer [3]. |
The Well Project. (2018). Hepatitis B. Retrieved from https://www.thewellproject.org/hiv-information/hepatitis-b
|
Hepatitis B Virus Infection
Viruses work by inserting their own genes into the host cells to replicate and spread though the tissue [3]. Hepatitis B is a double-stranded DNA containing virus and as such it is capable of inserting itself directly into the host cell's DNA [3]. This insertion causes hepatocyte injury, cirrhosis, chronic inflammation causing scar tissue formation and continuous liver tissue regeneration [3]. Continuous formation of damaged tissue and increased liver cell turnover causes an accumulation of mutations in the liver cells, resulting in cancer [3]. On the other hand, specifically with hepatitis B, there does not have to be cirrhosis for liver cancer to form [3]. The viral DNA insertion may cause enough disturbance in the liver cells to cause carcinoma [3]. |
Childs-kean, M. L., Deemer, K., & Madruga, C. (2018). Advances in hepatitis C treatment. Retrieved from https://www.drugtopics.com/clinical-news/advances-hepatitis-c-treatment
|
Hepatitis C Virus Infection
This disease is similar to hepatitis B but instead of a double-stranded DNA virus, Hepatitis C is a single-stranded RNA containing virus [3]. This means the virus does not insert itself directly into the liver cells DNA [3]. The presence of the virus causes changes to the cells resulting in inflammation, cell death, cell replication and cirrhosis [3]. |
Overall, the main cause of liver cancer is changes to the liver affecting the genetics or tissue of the organ which in turn results in abnormal structure and function [3]. These changes allow carcinoma to form [3].
Statistics
Incidence
In 2013, it was estimated that there would be 2100 new cases of liver cancer with 1550 being in males and 490 in females [5]. In comparison ,in 2017, there was an estimation of 2500 new cases of liver cancer [4]. 1900 of these cases involved males where as the other 580 cases occurred in females [4]. Thus, the incidence of liver cancer in Canada is steadily rising.
Mortality
An estimated 1000 people were expected to pass away due to liver cancer in 2013, 780 of which were estimated to be male and 240 of them female [5]. In contrast, the mortality estimates for 2017 were a total of 1200 people (950 males and 270 females) [4]. Not only has there been in increase in the incidence but also in the mortality estimates in the past 4 years.
Morbidity
As of January 2009, it is believed that 2985 people who were diagnosed with liver cancer 10 years ago are still alive [4]. Additionally, another 3750 people who have been diagnosed with liver cancer 2-5 years ago are still alive as well [4]. Thus, it is estimated that 6735 people in Canada are living with liver cancer as of 2009 who were diagnosed at least 2 years ago [4].
Developmental Considerations
The overall probability of someone developing liver cancer within their lifetime is 0.8% or 1 in 127 for males and 0.3% or 1 in 359 in females [4]. The greatest risk of developing liver cancer begins at the age of 40 and continues to increase with age [4]. However, this does not mean that it is impossible for children to develop liver cancer still [4].
In 2013, it was estimated that there would be 2100 new cases of liver cancer with 1550 being in males and 490 in females [5]. In comparison ,in 2017, there was an estimation of 2500 new cases of liver cancer [4]. 1900 of these cases involved males where as the other 580 cases occurred in females [4]. Thus, the incidence of liver cancer in Canada is steadily rising.
Mortality
An estimated 1000 people were expected to pass away due to liver cancer in 2013, 780 of which were estimated to be male and 240 of them female [5]. In contrast, the mortality estimates for 2017 were a total of 1200 people (950 males and 270 females) [4]. Not only has there been in increase in the incidence but also in the mortality estimates in the past 4 years.
Morbidity
As of January 2009, it is believed that 2985 people who were diagnosed with liver cancer 10 years ago are still alive [4]. Additionally, another 3750 people who have been diagnosed with liver cancer 2-5 years ago are still alive as well [4]. Thus, it is estimated that 6735 people in Canada are living with liver cancer as of 2009 who were diagnosed at least 2 years ago [4].
Developmental Considerations
The overall probability of someone developing liver cancer within their lifetime is 0.8% or 1 in 127 for males and 0.3% or 1 in 359 in females [4]. The greatest risk of developing liver cancer begins at the age of 40 and continues to increase with age [4]. However, this does not mean that it is impossible for children to develop liver cancer still [4].
References
- Forner, A., Reig, M., & Bruix, J. (2018). Hepatocellular Carcinoma. Lancet, 391(10127), 1301-1314. Retrieved from https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(18)30010-2.pdf.
- Huether. S.E., & McCance, K.L. (2017). Understanding Pathophysiology (6th edition). Brashers, V.L., & Rote, N. S. (Eds.). St. Louis, MO: Elsevier.
- Sanyal, A. J., Yoon, S. K., & Lencioni, R. (2010). The Etiology of Hepatocellular Carcinoma and Consequences for Treatment. The Oncologist, 15(Suppl 4), 14-22. Retrieved from http://theoncologist.alphamedpress.org/content/15/suppl_4/14.long.
- Cancer Statistics Canada (2017). 2017 Statistics. Retrieved from http://www.cancer.ca/en/cancer-information/cancer-101/canadian-cancer-statistics-publication/past-editions-canadian-cancer-statistics/?region=on.
- Cancer Statistics Canada (2013). 2013 Statistics. Retrieved from http://www.cancer.ca/en/cancer-information/cancer-101/canadian-cancer-statistics-publication/past-editions-canadian-cancer-statistics/?region=on.
- Balogh, J., Victor III, D., Asham, E. H., Gordon, S., Burroughs, Boktour, M., Saharia, A., Li, X., Ghobrial, R. M., & Monsour Jr, H. P. (2016). Hepatocellular Carcinoma: a review. Journal of Hepatocellular Carcinoma, 2016(3), 41-53. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5063561/.
- Burra, P., Zanetto, A., & Germani, G. (2018). Liver Transplantation for Alcoholic Liver Disease and Hepatocellular Carcinoma. Cancers, 10(2), 1-16. Retrieved from https://www.mdpi.com/2072-6694/10/2/46.
Image References
Loughborough University. (2019). Overweight men needed for study that looks at liver health and diabetes. Retrieved from https://www.lboro.ac.uk/news-events/news/2019/march/overweight-men-needed-for-liver-study/
